States are navigating a period of shifting fiscal conditions as revenue growth moderates, federal policy changes take effect, and long-term cost pressures persist. In this policy webinar, CSG South examined the fiscal landscape facing states and the factors shaping budget decisions during the 2026 legislative session.
Midwestern state legislators in their first four years of service are encouraged to apply for a 2026 fellowship to take part in the Bowhay Institute for Legislative Leadership Development (BILLD). More than 1,000 current and former lawmakers are BILLD graduates; alumni of the program include several top current state legislative leaders and others now serving in the U.S. Congress.
State agencies face a growing volume of sophisticated cyber threats that can disrupt operations and compromise sensitive data. To examine these issues, CSG South convened a panel discussion that explored how cyber threats to state government are evolving, which systems are most at risk, and what trends officials should monitor as adversaries refine their tactics.
The Council of State Governments is visiting state capitols across the Midwest in early 2026 to discuss CSG’s programs and services with the region’s legislators, other policy leaders and staff. CSG would like to meet with you.
Illinois and Ohio lawmakers overhauled their states’ energy policies in 2025, choosing different paths to the same destination: increasing electricity generation to meet skyrocketing demand.
In May, Nebraska will become the first state to implement provisions in a 2025 federal law that mark one of the biggest changes in the 61-year history of Medicaid: requiring some enrollees to participate in work-related activities. Across the country, minus a state securing a “good faith” extension waiver, these work requirements will take effect in January 2027.
They apply to the public health insurance program’s “expansion population” — low-income, able-bodied adults between the ages of 19 and 64. They also mean new obligations for states.
And in the not-so-distant future, there will be added fiscal responsibilities and restraints for states under the federal law (HR 1 of 2025), especially among the 40 that have expanded Medicaid eligibility. For example, many states have come to rely on provider taxes to help finance their share of Medicaid; federal constraints on this revenue source either have taken effect or will do so soon.
“HR 1 is going to require action, much sooner than later, even if some of these provisions don’t take effect for a while,” says Edwin Park, a research professor at the Georgetown University McCourt School of Public Policy’s Center for Children and Families. “[States] can’t just wait until the last second to think how to deal with some of the federal revenue or the taxes going away or some of the implementation costs. They’re going to have to think now about what their revenues and spending look like over time.”
Big shift: Trends in Medicaid eligibility and spending
Nationwide, the number of people eligible for Medicaid has increased considerably over the past decade and a half as the result of actions taken by state legislators, governors and/or voters. Since congressional passage of the Affordable Care Act in 2010, states have had the option of extending Medicaid coverage to non-disabled adults with incomes of up to 138 percent of the federal poverty level and getting an enhanced federal funding match (currently 90 percent).
Most states have taken up the federal government on this offer.
In the Midwest, Medicaid expansion is now a decade or more old in Illinois, Indiana, Iowa, Michigan, Minnesota, North Dakota and Ohio. The expansions in Nebraska and South Dakota are more recent; they also were the result of voter-approved ballot measures rather than legislative action.
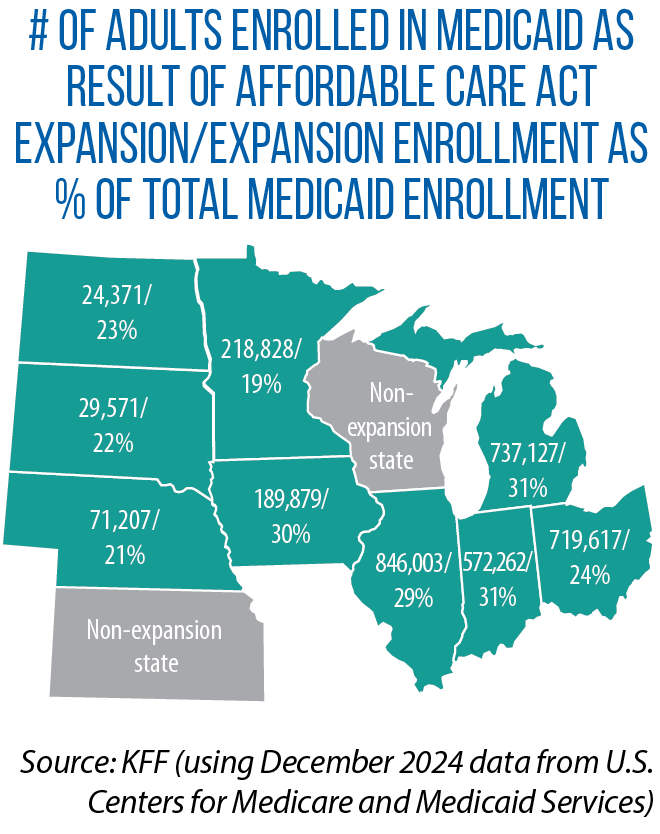
In Illinois, Rep. Anna Moeller says, uninsured rates fell 44 percent and hospitals saw a 37 percent reduction in uncompensated care immediately after the change in her state. Across all 50 states, the expansion population now makes up about one-quarter of all Medicaid enrollees, KFF data show (see map above for percentages for the Midwest). In 2024, one in five Americans reported getting health insurance through Medicaid.
According to the National Association of State Budget Officers, as of fiscal year 2024, 30 percent of state spending — states’ own dollars, plus federal revenue — was on Medicaid; that compares to 22 percent in FY 2010, prior to expansions under the Affordable Care Act.
HR 1 has the potential of changing these numbers and trends.
New era: Details on Medicaid work requirements
With the exceptions of Kansas and Wisconsin, all Midwestern states have adopted the Medicaid expansion. They must administer the new federal work requirements starting by early 2027. (Wisconsin also may have to comply because of coverage it provides via a federal waiver.) In an announcement of Nebraska’s first-in-the-nation implementation (set to begin in May), Steve Corsi, CEO of the state Department of Health and Human Services, hailed the change as a way of “encouraging greater economic and social participation.”
“Employment provides financial stability, fosters personal growth, and will help Nebraska’s small businesses in need of workers,” he said.
Similar sentiments, along with concerns about rising Medicaid costs, led some state legislatures to approve work requirements prior to enactment of HR 1. That includes Indiana (SB 2 of 2025), Iowa (SF 615 of 2025) and Ohio (HB 33 of 2023). South Dakota voters approved a ballot measure in 2024.
Actual implementation, however, will be new to all states in this region.
Outside the Midwest, a few states have carried out their own Medicaid work requirements, and those experiences point to a big challenge ahead: enforcing the federal rules while minimizing coverage losses among Medicaid-eligible individuals in the expansion population. In Arkansas, Park says, “people who should have been exempted from the work requirement or who met the work requirement” still lost coverage due to obstacles in reporting and documenting eligibility. In Georgia, “most of the lower-than-expected enrollment [in a Medicaid expansion] has been attributed to red tape associated with the work requirements.”
Many exemptions, eligibility pathways in federal law
Under HR 1, individuals in the expansion population must show they have worked 80 hours per month or, alternatively, have participated in job training, education programs or community service. States must verify compliance when an individual applies for Medicaid, as well as redetermine eligibility at least once every six months. The federal law provides a host of exemptions from this work requirement — for those who are medically frail, disabled veterans, pregnant women, parents and guardians of children up to age 13, caregivers for disabled individuals, recently incarcerated individuals, and people receiving treatment for a substance-use disorder.
States also can provide a “short-term hardship exception” to residents of high-unemployment counties (a jobless rate of 8 percent or more or 1.5 times the national average).
“We know from data analysis that most individuals subject to the work requirements may already be working or may be eligible for some type of exemption,” notes Robin Rudowitz, vice president at KFF and director of its Program on Medicaid and the Uninsured.
KFF found that, as of 2023, nearly two-thirds of Medicaid-covered adults between the ages of 19 and 64 were working. Among those not working, nearly three in 10 qualified for an exemption.
On paper, then, work requirements will be met or not apply to most individuals in the expansion population. However, the paperwork — the need for documentation and verification — can keep individuals from being enrolled in or remaining on Medicaid.
In Illinois, state health officials have told legislators that anywhere from 270,000 to 500,000 people in the state will lose Medicaid coverage as a result of the work requirements.
Rep. Anna Moeller
On the high side of the estimate, “that’s about 15 percent of current enrollees,” says Moeller, who is chair of the Illinois House Medicaid Subcommittee and co-chair of The Council of State Governments’ Midwestern Legislative Conference Health & Human Services Committee. “Just because people lose access doesn’t mean they stop getting sick; those costs get shifted to hospitals and emergency rooms and clinics,” she says. “Somebody has to end up paying for that care.”
Heavy implementation lift
Implementation of the work requirements, along with other rules related to compliance and more frequent checks on eligibility, is adding significant administrative burdens in Illinois, Moeller says. That includes a buildup of staff capacity, more communication and training with local partners, and upgrades in information technology. As part of HR 1, $200 million is available for states to establish systems around the new work requirements.
“To the extent that states can make it easy for people, and do things like data matching and not make individuals produce documentation, that certainly will be helpful in maintaining coverage,” Rudowitz says.
With data matching, states can automate at least the redetermination and renewal process. Information from other state benefit programs or workforce databases are accessed and eligibility proceeds ex parte, meaning enrollees don’t need to provide documentation or fill out forms.
“There are a lot of system changes that need to happen to do that data matching,” Rudowitz says. “No states are really set up right now to meet the new requirements. It’s a challenge of systems, timing, lack of guidance, staff capacity, all of these things.
“So even in those states that want to make it easy or want to be able to maintain coverage, there will be challenges in getting their systems and processes up to date.”
In an analysis for the first three months of 2025, Georgetown University researchers reviewed the share of renewals done ex parte in all states; percentages in the Midwest ranged from highs of 81.9 percent and 72.6 percent in Ohio and Minnesota, respectively, to lows of 17.2 percent and 17.3 percent in South Dakota and Nebraska, respectively.
Minnesota in recent years partnered with Code for America to improve the ex parte renewal process among aged, blind and disabled Medicaid enrollees. The result, according to Code for America, was a significant reduction in caseworker time as well as enrollees being renewed without having to take any action.
“If a state is wanting to reduce the enrollment loss that otherwise would happen, you certainly want to make the system as automated as possible, with as little burden as possible on individuals and families,” Park says. He adds, though, that provisions in HR 1 might point states “in the opposite direction of that approach.” Starting in October 2029, penalties will be imposed on states for erroneous payments or overpayments. The penalties apply to states with an error rate exceeding 3 percent.
“If you’re a state looking ahead, you will want to be designing systems that minimize what the federal government perceives to be an eligibility error,” Park says.
New fiscal restraints
As HR 1 advanced through the U.S. Congress, one option considered, but not ultimately included, was to end the enhanced federal matching rate of 90 percent for the Affordable Care Act expansion. (The traditional federal match ranges from 50 percent to 77 percent, according to KFF.) The enhanced match has made Medicaid expansion more fiscally (and politically) feasible in many states.
States, too, have “trigger laws” that tie continuation of the Medicaid expansion to the enhanced rate. Ohio included such a trigger in its latest budget (HB 96 of 2025). According to Georgetown’s Center for Children and Families, three other Midwestern states have these trigger laws. Statutory language in Illinois and Indiana would end the expansion; Iowa’s trigger provision provides “more flexibility” on the state response. South Dakotans will vote on a trigger law in November.
One sure new fiscal restraint coming to states under HR 1 is new limits on the use of provider taxes.
“Even though they are restrictions on state behavior,” Park explains, “they produce savings [for the federal government] because the assumption is that states aren’t going to be able to replace those lost revenues.”
If a state spends less on Medicaid, the federal government has less to match.
Every state but Alaska imposes at least one of these provider taxes on hospitals, nursing homes, intermediate care facilities for individuals with disabilities, and/or managed-care organizations, according to the National Association of State Medicaid Directors. Nationwide, provider taxes account for about 18 percent of the non-federal share of state Medicaid spending. State general funds make up nearly all of the remaining non-federal share, according to KFF.
Under HR 1, states cannot establish new provider taxes or increase the rates of existing ones. These restrictions cover all states, regardless of whether they expanded Medicaid.
“It’s hard to assess the impact because we don’t know what states may have moved forward with more provider taxes” if they had been allowed to do so, Rudowitz says.
But past practice in many states has been to raise or expand provider taxes during economic downturns, she says, as a means of maintaining Medicaid coverage and provider payments when state budgets are under duress and the availability of state general funds is limited. This option no longer exists.
Park notes, too, that provider taxes have been used by some states to expand their Medicaid programs.
Shrinking provider taxes
Another piece of HR 1 applies only to the Medicaid expansion states’ use of provider taxes. For those states, the federal government will phase in stricter limits on what’s known as the “safe harbor threshold.”
“Safe harbor” refers to states being able to get a federal match of Medicaid dollars from revenue generated by the provider tax. Right now, the tax threshold is 6 percent of a provider’s net patient revenue. In expansion states, though, that threshold declines by half of a percentage point in each fiscal year starting in FY 2028 before reaching 3.5 percent in FY 2032. (Provider taxes on nursing homes and intermediate care facilities are exempt.)
A KFF analysis shows that seven Medicaid expansion states in the Midwest — Illinois, Indiana, Iowa, Michigan, Minnesota, Nebraska and Ohio — impose a provider tax on hospitals exceeding that 3.5 percent threshold. An Illinois provider tax on managed care organizations also is higher than 3.5 percent.
“There’s a little bit of a lag on when these provisions go into effect,” Rudowitz says, “but this is going to be a big issue for state budgets.”
In Illinois, legislators have been told that HR 1 will result in a cumulative loss of $6.6 billion between FY 2028 and 2031 due to mandatory cutbacks in the provider tax and reduced federal support.
The federal changes are coming after a period in which many states moved ahead not only with the Medicaid expansion, but other policies to enhance benefits or boost access to behavioral health and various long-term-care options, Rudowitz says.
She adds that “states already have been facing a lot of cost pressures on the Medicaid side — pressures to increase provider rates, address inflation and workforce challenges.”
One area to watch in particular is state funding of home health care, Rudowitz says. Home- and community-based services account for a large portion of Medicaid spending, but providing these services is optional.
“They are expensive services, and they’re not required by the [federal] statute,” she says. “So we could see states wind up having to ratchet back or make changes to some of these home health care programs. And that could affect people who need the care or the payments to the providers.”
In support of its work on behalf of The Council of State Governments’ Midwestern Legislative Conference Health & Human Services Committee, CSG Midwest has developed two analyses on the impacts of HR 1 on the 11 states in the Midwest, with a particular focus on direct fiscal effects in two safety-net programs: Medicaid and the Supplemental Nutrition Assistance Program, or SNAP. This analysis on HR 1 and Medicaid was produced in December 2025. The first analysis was released in July 2025 and focuses on changes that will affect state administration and funding of SNAP. It can be found here.
Communities of the Midwest have long relied on volunteer firefighters and other emergency first responders. Another commonality stretching across state lines: concerns about the loss of these volunteers as retention and recruitment challenges mount. Demands on time. Increased training requirements. Aging populations. Those are among the biggest obstacles to securing an adequate number of volunteer firefighters and emergency responders, according to the U.S. Fire Administration.
Term limits is coming back to the ballot in two Midwestern states, this time as the subject of two legislatively referred constitutional amendments approved in 2025 by the Nebraska and North Dakota legislatures. Both measures seek to alter, rather than abolish, legislative term limits previously approved by voters in those two states.
Nebraska’s law dates back 25 years and prevents members of the Unicameral Legislature from serving more than two consecutive, four-year terms in office. The proposed constitutional amendment would allow up to 12 years of consecutive legislative service. “By adding one term to the current term limit, we can allow senators to represent their constituents [when] they’re most knowledgeable and effective,” Nebraska Sen. Robert Dover, the sponsor of LR 19CA, said in committee testimony.
Sixteen U.S. states currently have legislative term limits. The most recent such law was enacted by North Dakota voters in 2022 — a lifetime cap of eight years in the House and eight years in the Senate. Under the change being sought by legislators, members could serve up to four four-year terms, amounting to a total of 16 years, regardless of legislative chamber.
In his floor testimony in favor of SCR 4008, North Dakota Sen. Michael Dwyer said his work as a legislator has been positively impacted by the guidance of more-experienced colleagues. Allowing members to serve longer in the House or Senate will allow this kind of legislator-to-legislator mentoring and support to continue, he said.
Michigan voters changed the state’s term-limits law in 2022, supporting a legislatively referred constitutional amendment. The previous law had set lifetime limits of three two-year terms in the House and two four-year terms in the Senate. Now, the lifetime cap is set at 12 years (instead of 14), but all of those years can be spent in a single chamber. Legislators sought this tweak, in part, to allow for more legislative continuity and institutional knowledge in each chamber.
Capital Closeup is an ongoing series of CSG Midwest articles focusing on institutional issues in state governments and legislatures.
Starting in the latter part of 2026, Illinois will begin allowing terminally ill, mentally capable adults to obtain and self-administer medication to end their lives. Legislators passed SB 1950 during the fall 2025 veto session of the Illinois General Assembly; Gov. JB Pritzker signed the measure in December.
According to the advocacy group Death with Dignity, similar bills were passed in 2025 by legislatures in Delaware (signed into law) and New York (awaiting a decision by the governor as of early December). Illinois became the 12th U.S. state, and first in the Midwest, with such a law.
Under SB 1950, individuals with a prognosis of six months or less to live can request a prescription for aid-in-dying medication. The oral and written requests can only be made by the patient to the patient’s attending physician. SB 1950 includes language for what that written request should entail. (A written, signed request is required.)
The attending physician’s duties include determining the mental capacity of the patient (with referral to a mental health profession if warranted), confirming that coercion did not play a role in the request, providing information on other end-of-life treatment options, and referring the patient to a consulting physician for medical confirmation. No health care provider is required to participate, and SB 1950 makes it a felony to coerce anyone to request the medication or to forge a request.
The Illinois Department of Public Health will produce annual reports on the number of prescriptions for aid-in-dying medication, the number of physicians who prescribed it, and the number of deaths. Oregon’s Death With Dignity Act was the first of its kind in the nation and dates back to 1997. In 2024, there were 607 recipients of aid-in-dying medication in Oregon and 376 deaths. The number of deaths under the Oregon law has risen over time — from 42 in 2003, to 73 in 2014, to a high of 386 in 2023 (followed by the slight decline in 2024).
Over the past five years, these measures have been introduced but not passed in several Midwestern states: Indiana (HB 1011 of 2025), Iowa (SF 2101 and HF 2288 of 2024), Kansas (HB 2202 of 2021), Michigan (SB 681 of 2023), Minnesota (SF 3215 of 2025), and Wisconsin (AB 781 of 2024).
Canada has allowed eligible adults to request medical assistance in dying for nearly a decade. The federal law does not make eligibility contingent on a terminal illness; the criteria is having a “grievous and irremediable medical condition.” The aid-in-dying medication can be administered by either a health professional or the patient. In 2023, the number of medically assisted deaths in Canada reached a one-year high of 15,343 — 4.7 percent of all the country’s deaths that year.
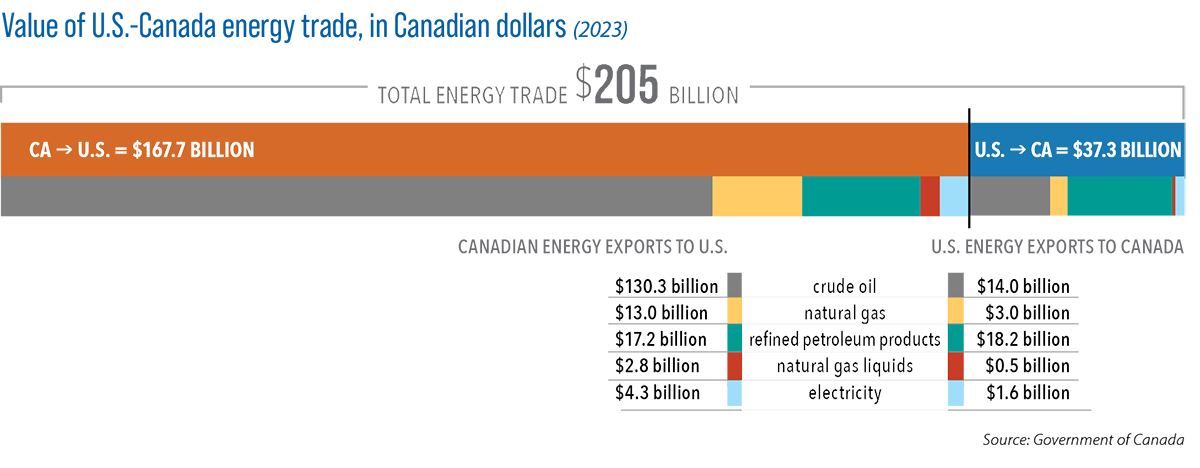
The U.S. and Canadian energy economies are inextricably intertwined. This Issue Brief explores the binational relationship in detail, with a focus on its implications for the states and provinces of The Council of State Governments’ Midwestern Legislative Conference. Several subject areas are covered:
The status of the relationship, in a year marked by threats of tariffs and counter tariffs and increased electrification in the United States and Canada.
A breakdown of today’s cross-border energy trade, with a look at what goods are traded to and from the United States and Canada. Detail is provided on some of the activity centered in the Midwest, including the movement of hydrocarbons via pipelines and electricity via cross-border transmission lines. Information on U.S. exports of biofuels to Canada also is included.
Projections of future electricity demand on both sides of the U.S.-Canada border, and how the binational energy relationship can help meet greater demand.
The possibility of a nuclear energy resurgence, as reflected in new laws and recent activity in Midwestern states and provinces. As energy demands shift, understanding the two countries’ binational relationship — and the potential for new or deeper connections in the future — is more critical than ever.
“Center of Power” was produced by the Midwestern Office of The Council of State Governments in support of two Midwestern Legislative Conference committees, Energy & Environment and Midwest-Canada Relations, as well as the 2025 MLC Chair’s Initiative of Saskatchewan Minister Lori Carr.
Minister Carr chose “North American Energy Security: Powering Our Future” as her 2025 MLC Chair’s Initiative. This subject has been the focus of various policy resources and programming for Midwestern legislators throughout 2025. The MLC also adopted a policy resolution in July 2025 on binational energy security and partnerships.





 They apply to the public health insurance program’s “expansion population” — low-income, able-bodied adults between the ages of 19 and 64. They also mean new obligations for states.
They apply to the public health insurance program’s “expansion population” — low-income, able-bodied adults between the ages of 19 and 64. They also mean new obligations for states.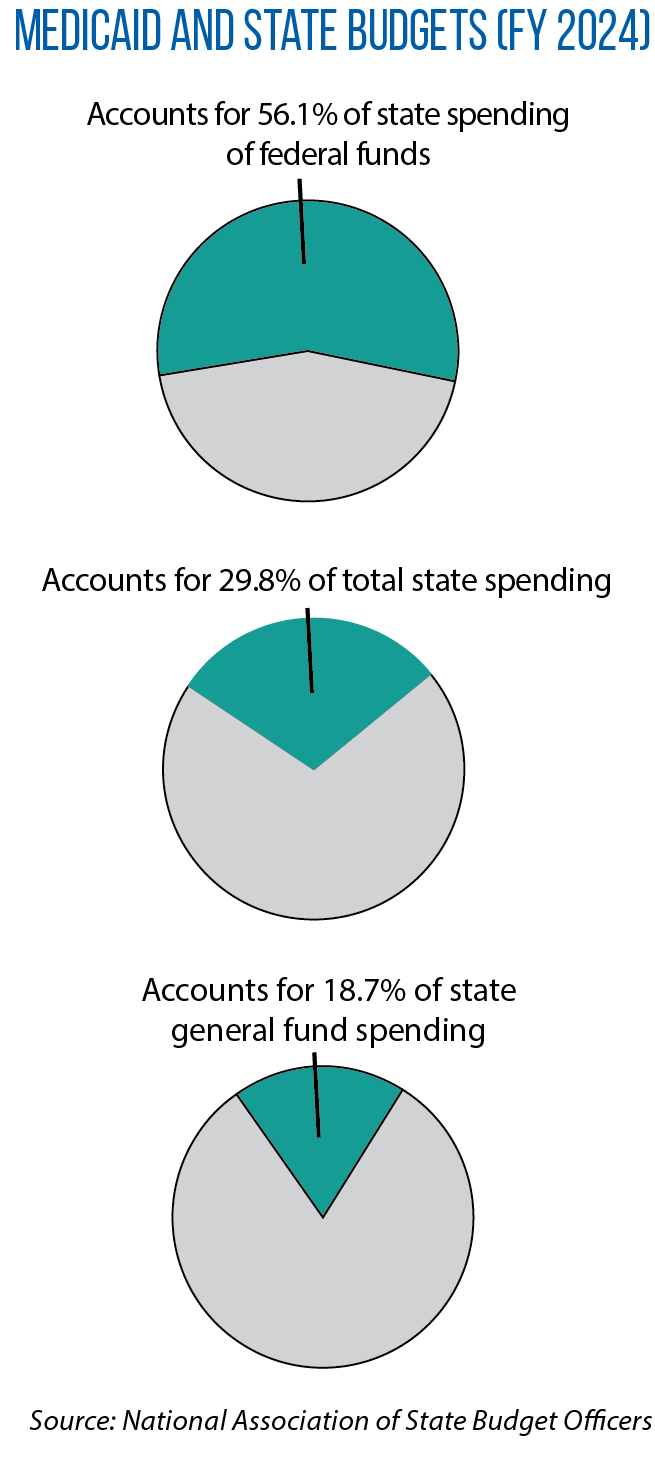 With the exceptions of Kansas and Wisconsin, all Midwestern states have adopted the Medicaid expansion. They must administer the new federal work requirements starting by early 2027. (Wisconsin also may have to comply because of coverage it provides via a federal waiver.) In an announcement of Nebraska’s first-in-the-nation implementation (set to begin in May), Steve Corsi, CEO of the state Department of Health and Human Services, hailed the change as a way of “encouraging greater economic and social participation.”
With the exceptions of Kansas and Wisconsin, all Midwestern states have adopted the Medicaid expansion. They must administer the new federal work requirements starting by early 2027. (Wisconsin also may have to comply because of coverage it provides via a federal waiver.) In an announcement of Nebraska’s first-in-the-nation implementation (set to begin in May), Steve Corsi, CEO of the state Department of Health and Human Services, hailed the change as a way of “encouraging greater economic and social participation.”
 With data matching, states can automate at least the redetermination and renewal process. Information from other state benefit programs or workforce databases are accessed and eligibility proceeds ex parte, meaning enrollees don’t need to provide documentation or fill out forms.
With data matching, states can automate at least the redetermination and renewal process. Information from other state benefit programs or workforce databases are accessed and eligibility proceeds ex parte, meaning enrollees don’t need to provide documentation or fill out forms. States, too, have “trigger laws” that tie continuation of the Medicaid expansion to the enhanced rate. Ohio included such a trigger in its latest budget (
States, too, have “trigger laws” that tie continuation of the Medicaid expansion to the enhanced rate. Ohio included such a trigger in its latest budget (
 Nebraska’s law dates back 25 years and prevents members of the Unicameral Legislature from serving more than two consecutive, four-year terms in office. The proposed constitutional amendment would allow up to 12 years of consecutive legislative service. “By adding one term to the current term limit, we can allow senators to represent their constituents [when] they’re most knowledgeable and effective,” Nebraska Sen. Robert Dover, the sponsor of
Nebraska’s law dates back 25 years and prevents members of the Unicameral Legislature from serving more than two consecutive, four-year terms in office. The proposed constitutional amendment would allow up to 12 years of consecutive legislative service. “By adding one term to the current term limit, we can allow senators to represent their constituents [when] they’re most knowledgeable and effective,” Nebraska Sen. Robert Dover, the sponsor of  Sixteen U.S. states currently have legislative term limits. The most recent such law was enacted by North Dakota voters in 2022 — a lifetime cap of eight years in the House and eight years in the Senate. Under the change being sought by legislators, members could serve up to four four-year terms, amounting to a total of 16 years, regardless of legislative chamber.
Sixteen U.S. states currently have legislative term limits. The most recent such law was enacted by North Dakota voters in 2022 — a lifetime cap of eight years in the House and eight years in the Senate. Under the change being sought by legislators, members could serve up to four four-year terms, amounting to a total of 16 years, regardless of legislative chamber. Under SB 1950, individuals with a prognosis of six months or less to live can request a prescription for aid-in-dying medication. The oral and written requests can only be made by the patient to the patient’s attending physician. SB 1950 includes language for what that written request should entail. (A written, signed request is required.)
Under SB 1950, individuals with a prognosis of six months or less to live can request a prescription for aid-in-dying medication. The oral and written requests can only be made by the patient to the patient’s attending physician. SB 1950 includes language for what that written request should entail. (A written, signed request is required.)